High tibial osteotomy (HTO) is a surgical procedure designed to correct abnormal mechanical load distribution in the knee joint by reducing pressure on the damaged area. It is primarily used for osteoarthritis localized in the medial compartment of the knee. By correcting leg deformity, it aims to relieve pain and extend the joint’s longevity. This procedure is especially considered for younger, active patients as a method to delay or avoid knee replacement surgery.
The surgical principle involves making a controlled cut in the upper part of the shinbone (tibia) to change its alignment, redirecting body weight from the damaged inner knee compartment to the healthier outer compartment. Applied in early-stage osteoarthritis and leg deformities, this method can help patients return to physical activity.
What is High Tibial Osteotomy (HTO)?
High tibial osteotomy is a joint-preserving surgical intervention that corrects abnormal load distribution in the knee. The term "osteotomy" means bone cutting, and "high tibial" refers to the upper tibia where the procedure is performed. Its main goal is to correct leg bowing known as "bow-leggedness" (genu varum), transferring excessive load from the medial side of the knee to the more robust lateral side.
Surgical planning begins with detailed analysis of the patient’s mechanical axis. During the procedure, the bone is reshaped and fixed using plates and screws. This method holds a significant place among techniques categorized under lower extremity deformity surgery.
Who Is a Candidate for HTO?
High tibial osteotomy is not suitable for everyone; patient selection is crucial for success. Ideal candidates are typically under 60 years old, lead active lifestyles, and experience activity-related knee pain. Osteoarthritis should be confined to a single compartment (usually the medial side), with healthy cartilage in the lateral compartment. Adequate knee range of motion and absence of significant ligament instability are also important.
Conversely, patients with systemic rheumatic diseases (such as rheumatoid arthritis), severe obesity, or widespread osteoarthritis across the entire knee are generally not candidates for this surgery.
Preoperative Evaluation and Preparation
Preoperative assessment includes a thorough physical examination and radiologic imaging. Weight-bearing long-leg X-rays (orthoroentgenograms) are used to assess mechanical axis and degree of deformity. MRI scans evaluate ligamentous structures, menisci, and cartilage condition within the knee. These studies allow precise measurement of the correction angle needed.
Patient’s general health, chronic diseases, and medications are reviewed before surgery. Smoking cessation is strongly advised as smoking negatively affects bone healing.
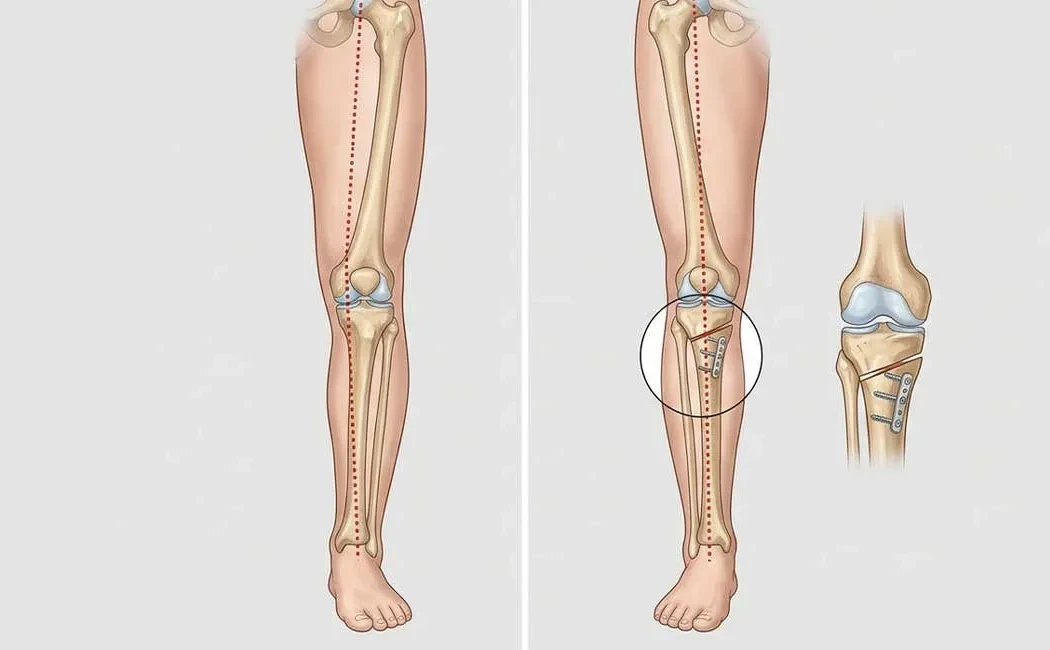
Surgical Procedure of High Tibial Osteotomy
The surgery is usually performed under general or spinal anesthesia and takes about 1-2 hours. The surgeon makes a small incision on the inner side of the upper tibia below the knee to access the bone. A precise cut (osteotomy) is made according to the planned correction angle, then the bone segments are opened and adjusted. The gap may be filled with bone grafts or synthetic materials.
The corrected bone position is stabilized with titanium plates and screws, providing rigidity until bone healing completes. Fluoroscopy (C-arm X-ray) guides the accuracy of correction during the procedure. Precision in surgical technique is critical to minimize postoperative complications.
Postoperative Recovery Process
The recovery phase is key to consolidating surgical success. Patients usually remain hospitalized for 1-3 days under observation. In the early weeks, movement is supported by crutches or a walker. Weight-bearing protocols depend on the type of osteotomy and fixation method, determined by the surgeon. During this period, performing exercises to protect joint health helps maintain muscle strength.
Bone healing generally takes 6-8 weeks, while return to full activity can span 3-6 months.
Physiotherapy plays a vital role in restoring knee range of motion and strengthening muscles. The rehabilitation protocol resembles post-knee replacement physical therapy but includes specific approaches focused on bone healing. Additionally, principles of nonunion surgery may be relevant for monitoring bone healing and managing delays. Postoperative wound care and dressing examples are shown below.
Risks and Complications of HTO Surgery
As with any surgery, high tibial osteotomy carries risks including infection, blood clots (deep vein thrombosis), nerve or vascular injury—although these are infrequent. A notable complication is delayed or improper bone healing at the osteotomy site. Such cases may require additional interventions like malunion surgery.
Insufficient or excessive correction can adversely affect knee mechanics. These risks are minimized by experienced surgical teams and careful planning. Patients should report symptoms such as infection signs or sudden increase in pain promptly, similar to vigilance advised for post-knee replacement complications.
Alternative Treatment Options
For patients not suitable for or opting out of HTO, various alternatives are available. Non-surgical options include weight loss, physical therapy, specialized knee braces, and intra-articular injections such as hyaluronic acid or platelet-rich plasma (PRP). Surgical alternatives encompass partial knee replacement (unicompartmental) or total knee replacement.
Knee replacement is generally reserved for older patients with widespread osteoarthritis, whereas HTO offers a joint-preserving, biological approach. The choice of treatment should be determined through detailed evaluation by an orthopedic surgeon specialized in joint-preserving surgeries. Our clinic also provides multidisciplinary care for other orthopedic areas such as bone tumors in children and treatment and treatment of hip impingement syndrome.
The information provided herein is for general informational purposes only and does not constitute medical advice. Decisions regarding high tibial osteotomy and other treatment options should be made following a thorough examination and appropriate diagnostic tests conducted by a qualified healthcare professional. Each patient's clinical condition may vary. Please consult a qualified medical professional for diagnosis and treatment. Do not delay seeking professional care based on the information provided.