Leg deformity correction is an extensive treatment process aimed at eliminating angular deformities of the lower extremities and restoring normal leg alignment. The deformities, medically known as genu varum (O legs) and genu valgum (X legs), are not merely cosmetic issues; if untreated, they may result in premature wear of the knee, hip, and ankle joints.
The primary goal in orthopedic surgery is to correct the weight-bearing mechanical axis to ensure balanced load distribution on the joints. This article reviews leg deformity correction, types of deformities, and contemporary treatment methods based on scientific evidence.
What Is Leg Deformity?
Leg deformity refers to the deviation of the femur and tibia bones from their normal anatomical axis. In a healthy individual, the mechanical axis passing through the hip, knee, and ankle follows a straight line. In deformities, this axis is disrupted, causing excessive load on certain parts of the joints and eventually cartilage damage.
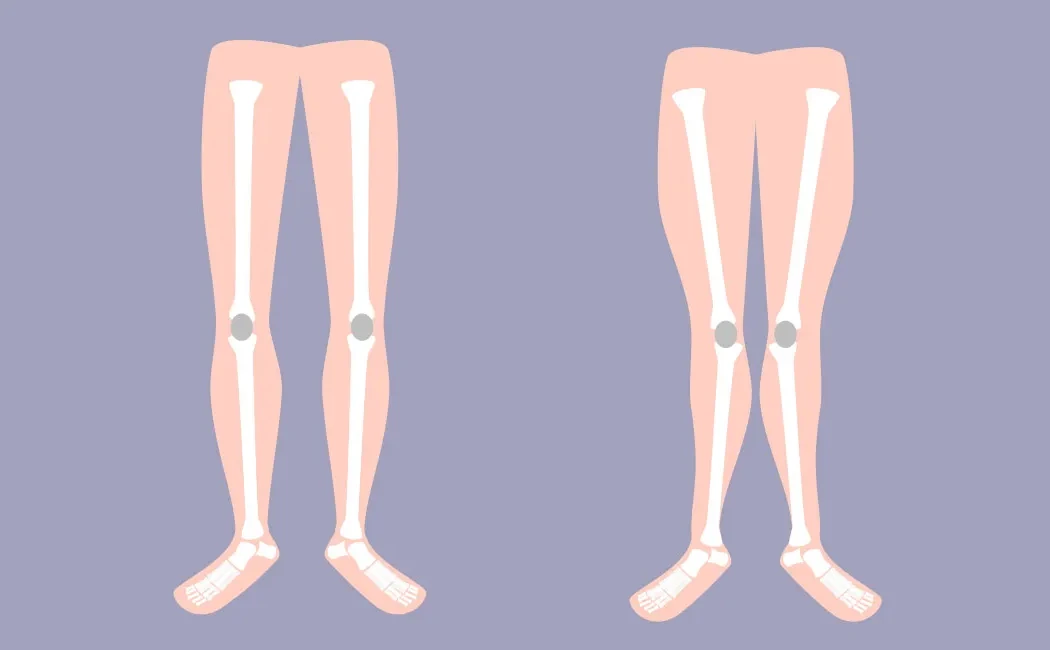
What Are Genu Varum (O Legs) and Genu Valgum (X Legs)?
Genu varum, commonly known as O legs, is characterized by knees that stay apart while the ankles touch. In this condition, the load concentrates more on the inner part (medial compartment) of the knee. Conversely, genu valgum (X legs) features knees that touch and ankles that remain apart, with load focusing on the outer part (lateral compartment) of the knee.
Physiological bowing in childhood typically improves with growth, while pathological deformities require treatment. For detailed information, please visit our page on O and X Leg Deformities in Children.
What Causes Leg Deformities?
Leg deformities can be congenital or develop later due to various factors. Understanding the underlying cause is critical for appropriate treatment planning.
Genetic and Developmental Factors
In some individuals, bone development can show angular deviations linked to genetic factors. Developmental disorders, such as Blount disease, arise from growth plate disturbances in the tibia leading to progressive leg deformities, generally manifesting in childhood. Learn more about Lower Extremity Deformities in Childhood.
Nutritional Deficiencies and Rickets
Deficiencies in vitamin D, calcium, or phosphorus can lead to bone softening and bending under body weight. Rickets is a common cause of leg deformities, especially in developing countries. In these metabolic conditions, surgical planning is not advised before correcting bone quality through metabolic treatments.
Trauma and Other Factors
Fractures involving growth plates or bone infections (osteomyelitis) can cause asymmetric growth, leading to secondary deformities. Malunited fractures may also disrupt the mechanical axis, resulting in leg deformity.
Symptoms and Diagnostic Process
Patients often present with cosmetic concerns, but leg deformities also cause functional impairments. Early diagnosis is essential to enable joint-preserving treatments.
Gait Abnormalities and Pain
In advanced deformities, patients may experience knocking knees during walking (X legs) or swaying from side to side (O legs). Over time, this may lead to knee, hip, or lower back pain, usually worsening with activity and easing at rest.
Physical Examination and Imaging Methods
During diagnosis, the physician analyzes the patient's gait and joint range of motion. Definitive diagnosis and surgical planning require full-length standing radiographs called orthoroentgenograms that include the hip, knee, and ankle.
Methods for Leg Deformity Correction
Treatment approaches depend on patient age, severity of the deformity, and associated conditions. Methods applied in lower extremity deformity surgery require a multidisciplinary perspective.
Non-Surgical Methods
Mild deformities in children can be monitored or managed with guiding devices such as hemiepiphysiodesis before more invasive interventions. In adults, non-surgical options rarely correct the deformity but may provide pain relief. Early-stage osteoarthritis can be managed with joint-preserving surgeries to delay the need for joint replacement.
Surgical Correction: Osteotomy and Ilizarov Method
Surgery is the main treatment for adults and patients with closed growth plates. Osteotomy involves cutting bone in a controlled manner to remodel alignment. Correction can be acute (single-step) or gradual using the Ilizarov method for deformity correction.
If leg length discrepancy is also present, bone lengthening surgery can be combined with deformity correction in the same procedure.
Postoperative Care and Recovery
Successful surgery must be followed by a disciplined rehabilitation program. Recovery times vary depending on the surgical technique used (plate and screws, intramedullary nail, or external fixation).
Physical Therapy and Rehabilitation
Early postoperative joint movement exercises begin in the initial phase. Weight bearing is determined by the surgeon based on radiological bone healing progress. Strengthening exercises are vital to adapt to the new mechanical alignment of the leg.
Complications and Precautions
As with any surgery, there are risks such as infection, neurovascular injury, or non-union. Adherence to postoperative instructions is crucial to prevent complications, especially those requiring reoperation for malunion. Smoking negatively affects bone healing and should be strictly avoided during recovery.
Expert Opinion and Information
Leg deformity correction surgery demands high technical precision. Prof. Dr. Halil İbrahim Balcı utilizes computer-assisted deformity analysis, gained from experience at international centers like the Paley Institute, to create personalized treatment plans. The goal is not only cosmetic improvement but also to preserve long-term joint health and enhance functional capacity.
This content is intended for general informational purposes only. It is essential to consult a specialist in orthopedics and traumatology for diagnosis and treatment. Each patient's condition is unique and requires a personalized assessment through a medical examination. The information provided on this site does not substitute professional medical advice, diagnosis, or treatment. Do not delay seeking professional care or disregard medical advice based on this content.