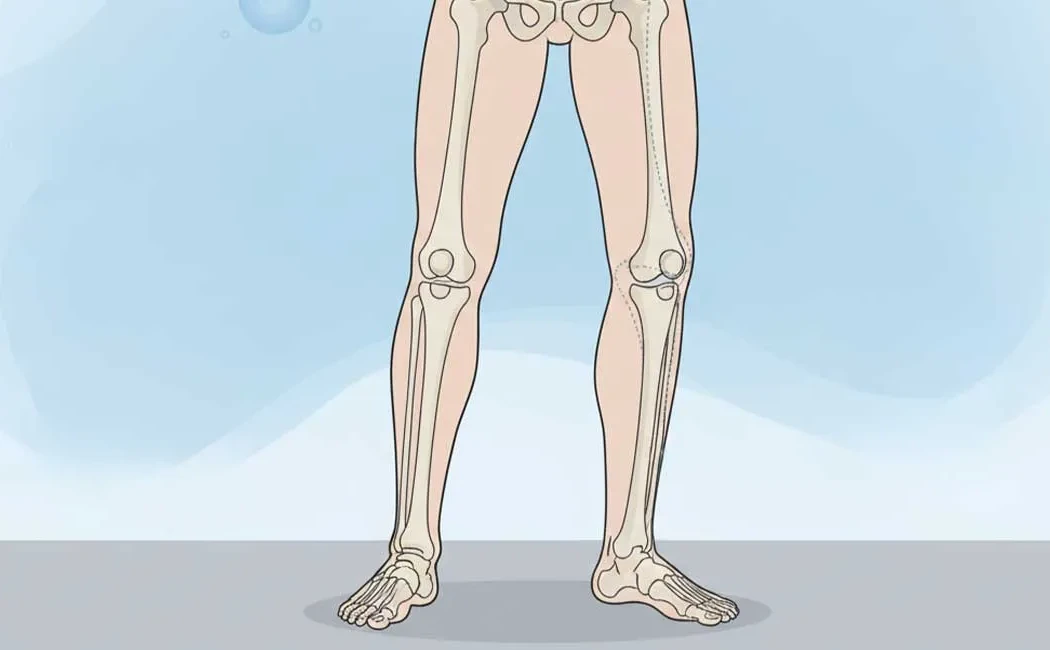
Knock-knee deformity, medically known as Genu Valgum, is characterized by an inward angulation of the legs at the knee level. In this condition, when standing, the knees touch each other while there is a visible gap between the ankles. This condition can cause both cosmetic concerns and functional problems. While sometimes considered a normal variation during childhood development, it may also become permanent due to various pathological causes.
Early diagnosis and appropriate treatment are crucial to prevent future joint damage. The condition of growth plates in children is a key factor guiding the treatment approach. This article provides comprehensive information on the causes of knock-knee deformity and the latest treatment methods.
What is Knock-Knee Deformity (Genu Valgum)?
Genu Valgum is a deformity where the mechanical axis of the lower limb is altered. In a normal leg, the weight-bearing axis runs in a straight line through the center of the hip, knee, and ankle. In knock-knee deformity, more load is placed on the outer compartment of the knee (lateral side). This can eventually lead to meniscus tears, cartilage wear, and early-onset osteoarthritis.
Causes of Knock-Knee Deformity
The development of this deformity may be due to a single cause or a combination of factors. Physiological growth processes are common causes in children, whereas metabolic bone diseases are more prominent in pathological conditions.
Common causes include:
- Genetic Predisposition: Family history of similar deformities can increase risk.
- Metabolic Disorders: Vitamin D deficiency causing rickets can lead to bone softening and deformity.
- Trauma and Infections: Fractures or infections affecting growth plates (osteomyelitis) may cause asymmetrical growth and deformity.
- Obesity: Excess body weight increases the load on developing joints, exacerbating knee angulation.
The variety of underlying causes directly influences treatment decisions. For a broader perspective, you can refer to our article on common deformities in children and the importance of early intervention.
Symptoms and Diagnostic Methods
Patients often present with cosmetic concerns, but Genu Valgum may also produce functional symptoms. The most noticeable symptom is the knocking of knees during walking, which leads to difficulty in gait. Advanced cases may experience pain around or in front of the knees, quick fatigue, and difficulty in running activities.
Physical examination is fundamental to diagnosis. The doctor measures the contact between the knees and the distance between the ankles (intermalleolar distance) while the patient is standing. Definitive diagnosis and degree of deformity are established through standing full-leg radiographs, known as orthoroentgenograms, which show the entire leg from hip to ankle.
Prevalence and Developmental Process in Children and Adults
Children’s leg appearance naturally changes during growth. Infants are typically born with a slight bow-legged (Genu Varum) appearance. Around 18-24 months, leg alignment normalizes, followed by a physiological knock-knee angle typically appearing between ages 3 to 4. This usually self-corrects by ages 7 to 8, reaching the normal adult alignment.
Persistent knock-knee deformity outside expected age ranges or unilateral deformities are pathological and require specialist evaluation. Our page on lower limb deformities and treatment methods in childhood provides detailed information on this developmental course and indications for intervention.
Treatment Methods for Knock-Knee: Surgical and Non-Surgical Options
Treatment depends on the patient’s age, severity of deformity, and underlying cause.
Non-Surgical Methods (Conservative Treatment)
Mild, physiologic cases typically require observation only. Metabolic problems such as Vitamin D deficiency are managed with medication. Weight management and muscle-strengthening exercises may support correction. The following image illustrates recommended physical therapy exercises for this condition.
Surgical Treatment Methods
Surgery may be necessary if conservative methods fail or in cases of severe deformity. Surgical options can be divided into two main types:
1. Guided Growth (Hemiepiphysiodesis): Used in children with open growth plates. The growth plate on the inner side of the knee is temporarily slowed, allowing the outer side to grow normally and gradually correct the deformity. This is a minimally invasive procedure.
2. Corrective Osteotomy: Applied to adults with mature bones or older adolescents. The bone is surgically cut and realigned, then fixed with plates, screws, or external fixators.
Understanding the surgical steps can help patients be better prepared. The flowchart below summarizes the steps involved in knock-knee surgery.
For more detailed information on surgical techniques, visit our pages on lower limb deformity surgery and knock-knee and bow-leg deformity treatments. To learn about possible rare complications during recovery after surgery, see nonunion issues in bone fractures and treatment approaches.
Technological advancements have enhanced surgical planning accuracy. The role of robotic technologies in deformity surgery is increasingly significant.
Factors Affecting Treatment Choice and Success
Treatment success depends on proper patient selection and timing. Early interventions generally allow less invasive approaches. The importance of age in deformity surgery is significant; children with remaining growth potential have higher correction capacity.
In adults, long-standing untreated deformities may result in joint arthritis. In these cases, deformity correction alone may be insufficient, and joint replacement could become necessary. For patients with advanced joint damage, post-knee replacement care and common issues should also be considered in treatment planning.
This content has been prepared by Prof. Dr. Halil İbrahim Balcı for general informational purposes only and does not constitute medical advice. The information provided is not intended to replace individualized diagnosis, treatment, or professional guidance. Diagnosis and treatment should be determined solely after a face-to-face examination by a qualified physician, as each patient's clinical condition is unique. For any health-related concerns, please consult a specialized healthcare professional without delay.