Non-union fractures are considered one of the most challenging problems in orthopedic surgery. Failure or inadequate healing of the fracture significantly affects patients’ quality of life, prolongs treatment durations, and increases the risk of complications. In this context, the use of external fixators stands out as an effective method in managing non-union fractures.
Definition and Causes of Non-Union Fractures
Non-union refers to the failure of the bone ends at the fracture site to unite, causing a halt in the healing process. Clinically, it is usually defined as the absence of healing within 6 to 9 months. Causes of non-union can be categorized into biological and mechanical factors. Biological factors include inadequate periosteal blood supply, infection, smoking, poor nutrition, and concurrent systemic diseases such as diabetes. Mechanical factors involve insufficient stability at the fracture site, inappropriate surgical techniques, or early weight-bearing post-treatment.
Definition and General Use of External Fixators
External fixators are devices applied externally to bones and soft tissues to stabilize the fracture area. They can be in the form of ring systems like the Ilizarov or monolateral rods. These systems are preferred because of their minimally invasive application, easily adjustable stability, and suitability for use in infected or soft tissue-compromised regions.
Use of External Fixators in Non-Union Fractures
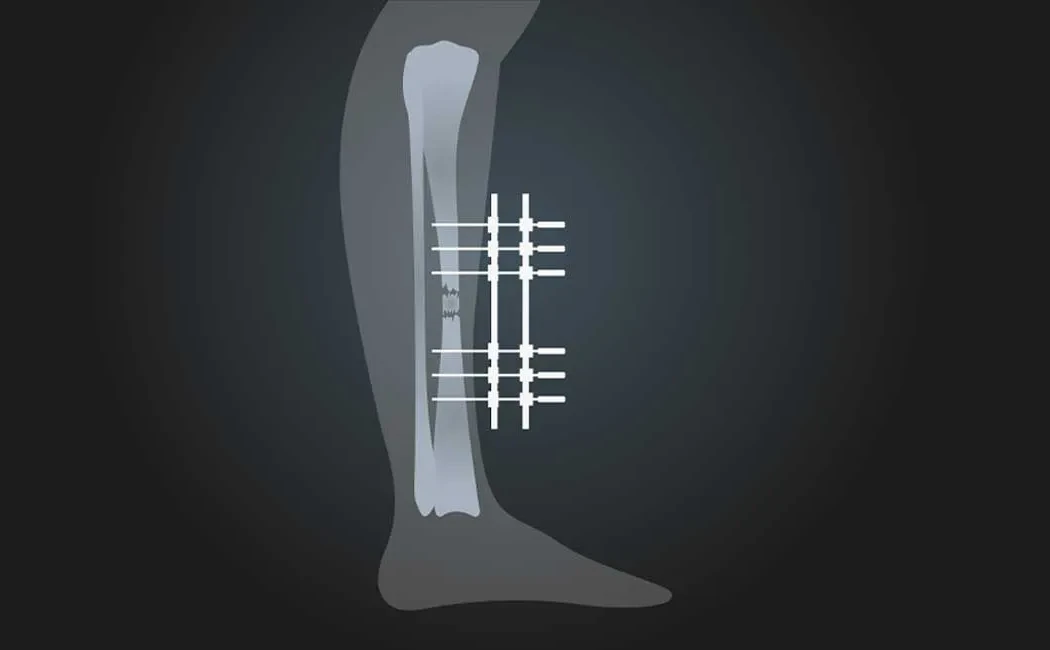
The primary goal of applying external fixators in non-union fractures is to provide mechanical stability at the fracture site and promote biological healing. External fixators control micromovements at the bone ends, creating an optimal mechanical environment. This preservation of local blood flow supports osteogenesis.
Surgical Techniques
In the treatment of non-union fractures, infection focus is first evaluated and controlled. Then, the appropriate type and size of external fixator is selected for the fracture site. During application, deformities are corrected, and biological healing is facilitated through compression or distraction methods at the fracture line. The Ilizarov method not only corrects deformities but also allows for bone lengthening or reconstruction.
Healing Process and Follow-up
After external fixator application, patients are regularly monitored through clinical and radiological evaluations. The increase in bone formation at the fracture site is followed, and the stability of the device is assessed. A tailored rehabilitation program is implemented to ensure early preservation of function.
Advantages and Disadvantages
Major advantages of external fixators include their minimally invasive nature, ability to be used in infected areas, and adjustable stability. Additionally, the ability to regulate mechanical stability optimizes the healing process. Disadvantages comprise discomfort caused by the device, pin tract infections, and challenges related to prolonged use.
Scientific Data and Clinical Outcomes
Numerous studies in the literature demonstrate high success rates of healing in non-union fractures treated with external fixators. Treatments using the Ilizarov system significantly overcome the problem of non-union by supporting both mechanical and biological healing.
These methods show increased success with a multidisciplinary approach and appropriate patient selection. Outcomes improve in parallel with surgical experience and the patient’s overall health condition.
Ultimately, the proper indication and expert use of external fixators in non-union fractures improves patients’ functional recovery, positively influences the treatment process, and reduces complications.