Deformity surgery is a highly specialized field within orthopedics that involves correcting congenital or acquired malformations of the extremities, following anatomical and biomechanical principles. Angular deformities, rotational abnormalities, or limb length discrepancies not only pose aesthetic concerns but can also threaten joint health by leading to early osteoarthritis. As a result, precise analysis and surgical planning of deformities are imperative.
This discipline goes beyond simple bone realignment; it integrates the bone’s growth potential, soft tissue balance, and the patient’s functional expectations into a comprehensive assessment. Particularly, the CORA (Center of Rotation of Angulation) principle geometrically identifies the deformity’s origin and the precise correction point, acting as a roadmap for the surgeon. Thanks to advanced imaging technologies and modern surgical techniques, even the most complex deformities can now be managed effectively.
What is Deformity? Types and Causes
Deformity refers to any deviation of the musculoskeletal system from its normal anatomical structure. This deviation may present as bending in a single plane, rotation around the bone’s longitudinal axis, or shortening. Accurate classification of deformities is the first step toward defining an appropriate treatment strategy.
Congenital vs. Acquired Deformities
Deformities are broadly categorized by their origin into congenital and acquired groups. Congenital deformities are present at birth and are often caused by genetic factors or developmental issues during pregnancy. Conditions such as fibular hemimelia or congenital pseudarthrosis of the tibia fall into this category.
Acquired deformities result from external factors such as trauma, infection, metabolic diseases, or tumors occurring later in life. Pediatric fractures involving the growth plates are particularly significant, as improper healing can lead to severe angular deformities and limb length discrepancies. Malunions, where fractures heal incorrectly, remain one of the most common acquired deformity causes in adults.
Valgus, Varus, and Rotational Deformities
Deformities are named according to their orientation within anatomical planes. In the frontal plane (anterior view), inward angulation of the knees is referred to as "Genu Valgum" (knock knees), while outward angulation is known as "Genu Varum" (bow legs). These angular abnormalities are often accompanied by rotational deformities.
Rotational deformities typically manifest as in-toeing or out-toeing gait patterns. Such malalignments disrupt the biomechanics of the hip, knee, and ankle joints and may predispose to joint damage over time.
Understanding CORA (Center of Rotation of Angulation)
CORA is the cornerstone principle of deformity surgery, representing the geometric center of the bone’s deformity. Defined by Paley, this concept forms the mathematical foundation for surgical planning. Determining whether the deformity is unifocal (single point) or multifocal (multiple points) requires precise CORA analysis.
Definition and Geometric Principles of CORA
CORA is identified where the proximal and distal mechanical or anatomical axes of the bone intersect. Achieving ideal correction depends on performing the osteotomy (bone cut) exactly at this point. When osteotomy is done precisely at CORA, the deformity is corrected angularly, restoring the anatomical axis without displacement. If performed away from CORA, the bone ends must be translated to prevent creating a secondary, translational deformity. This geometric relationship is critical in deciding the surgical technique.
Methods for Identifying CORA
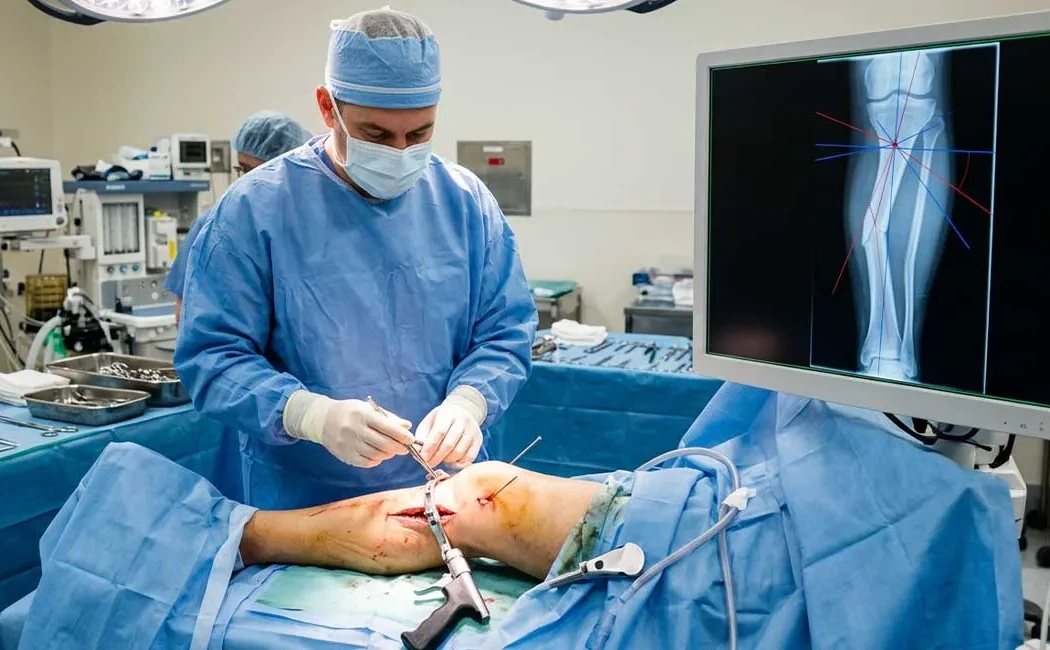
Locating CORA requires detailed radiological assessment, usually utilizing full-length standing radiographs with lines drawn to define the mechanical axes. The following diagram illustrates the step-by-step identification process, including preoperative and postoperative comparison.
Contemporary surgeries use digital software to measure CORA with millimetric accuracy. The proximity of CORA to joint surfaces or the diaphysis directly influences surgical approach and implant selection.
Principles of Deformity Correction Surgery
Deformity correction can be conducted through acute (single-stage) or gradual (multi-stage) methods. The choice depends on the deformity’s severity, soft tissue condition, and neurovascular status.
Angular and Mechanical Correction Methods
Acute correction is suitable for moderate deformities where soft tissues can tolerate immediate lengthening. The osteotomy is followed by internal fixation with plates, screws, or intramedullary nails. However, in severe deformities or when limb shortening coexists, acute correction carries risks such as nerve palsy or vascular complications. In such cases, staged correction methods (extremity deformity correction) are safer. Techniques tailored to the patient’s anatomy (lower extremity deformity surgery) ensure individualized care.
Ilizarov Method and Other Fixator Systems
Complex deformities requiring gradual correction often utilize circular external fixators like the Ilizarov frame or computer-assisted hexapod systems, considered gold standards. These devices allow controlled bone lengthening and angular adjustments at about 1 mm per day.
The Ilizarov technique preserves soft tissue integrity while enabling the treatment of severe deformities. It can be combined with bone lengthening procedures (bone lengthening surgery) to correct curvature and shortening simultaneously.
Surgical Planning: 3D Imaging and Personalized Approaches
Advances in technology have replaced estimations with precise, millimeter-based calculations in deformity surgery. Using CT data, 3D models enable surgeons to simulate procedures virtually.
This technology facilitates the production of patient-specific cutting guides, ensuring osteotomy is performed at the exact planned location and angle. 3D planning in deformity surgery reduces operative time, increases success rates, and lowers radiation exposure.
Postoperative Recovery After Deformity Surgery
The postoperative phase is as crucial as the surgery itself. Healing depends on bone union rates, fixation methods used, and patient compliance. The rehabilitation process is summarized in the flowchart below.
Patients typically begin physiotherapy soon after surgery. Those with external fixators require rigorous care of the device and pin sites to prevent infection. Full weight-bearing begins once radiographic signs confirm bone consolidation.
Complications: Nonunion and Malunion
As with any surgery, deformity correction carries risks. The most common complications include nonunion, where the bone fails to heal, and malunion, where healing occurs in an incorrect position. These issues often stem from inadequate biological or mechanical conditions.
Nonunion surgery involves interventions such as bone grafting or revision fixation. Successful management of nonunion (nonunion management in deformity surgery) requires optimizing biological and mechanical factors. If residual deformity exists or malunion recurs, malunion diagnosis and treatment protocols are applied, often requiring a corrective osteotomy.
Extremity Deformities in Children and Timing of Intervention
Pediatric deformity management differs from adults due to ongoing growth. Interventions involving growth plates (physiolysis) can support spontaneous correction (hemiepiphysiodesis) or, if misapplied, cause permanent damage. Thus, timing is critical: intervention may be delayed until growth completion or advanced early in progressive cases.
In conclusion, deformity surgery is a multifaceted process demanding detailed analysis, appropriate patient selection, and meticulous surgical technique. Planning based on CORA principles and a skilled multidisciplinary team significantly impacts patients’ functional recovery.
This content is intended for general informational purposes only and does not constitute professional medical advice, diagnosis, or treatment. If you have any health concerns or questions, you should consult a qualified healthcare professional or medical provider. The information provided here may not be applicable to your individual medical condition and should not replace the recommendations of your doctor. Medical conditions and treatments can vary from person to person.